


US Hospitals: In Sickness and in Hell
US hospitals continue to lose ground in their struggle to manage the escalating outbreak of the coronavirus COVID-19, now a global pandemic.


The World Health Organization finally declared on Wednesday that Coronavirus COVID-19 has become a pandemic.
This with now nearly 128,343 confirmed cases in 116 countries and 4,720 reported deaths—a case fatality rate (CFR) inching higher at 3.7%—according to Johns Hopkins CSSE.
US cases have swelled 10x in just over a week to 1,663 with 40 deaths, stats still more troubling because of continued under measurement caused by lack of testing more than two months since acknowledging the outbreak back in January.
But the most unsettling surprise has been the dangerous ineptitude of the US response as led and compounded by deliberate efforts of US President Trump to conceal and downplay risks from the virus which he views more as a threat to his reelection prospects.
Such failures continue to impair efforts by frontline US responders at hospitals struggling all over the country with poor data plus chronic shortages of virus testing kits and vital supplies plus loss of staff who have been sickened or must be quarantined after exposure to coronavirus patients.
For investors, the best odds are that rosy guidance for 2020 hospital operators released just weeks ago will be reduced on potentially dramatically lower profits as already low margin emergency rooms fill up with patients who may struggle to pay while high margin discretionary surgeries and treatments will be postponed.
Bonds in the largest US hospital operators HCA Holdings (HCA US), Tenet Healthcare (THC US), and Community Health Systems (CYH US), already generously priced on ambitious market expectations even before the COVID-19 outbreak, are increasingly vulnerable to meaningful downside pressure as the rapidly spreading virus overwhelms the country's severely underprepared capacity to cope.

A Pandemic Like None Before in History—Even For Trump
The outbreak already is notable for how badly it's been managed, particularly by Trump—a prolific liar who has aggressively spread false and confusing information throughout the crisis, even as recently as yesterday in his error-ridden address to the nation which he turned into another excuse to blame a crisis on "foreigners."
Par for the course for Trump, who in recent weeks claimed the coronavirus was a Democratic hoax aimed to hurt his reelection prospects, that it will go away naturally when the weather warms up in April (it won't), that the US will soon have a vaccine (doctors and scientists say more likely 12-18 months), that cases in the US "when you have 15 people (tally as of February 20), and the 15 within a couple of days is going to be down to close to zero. That’s a pretty good job we’ve done." Not really. US cases already were 4x higher to 60 on this day, February 26, and scaling rapidly.
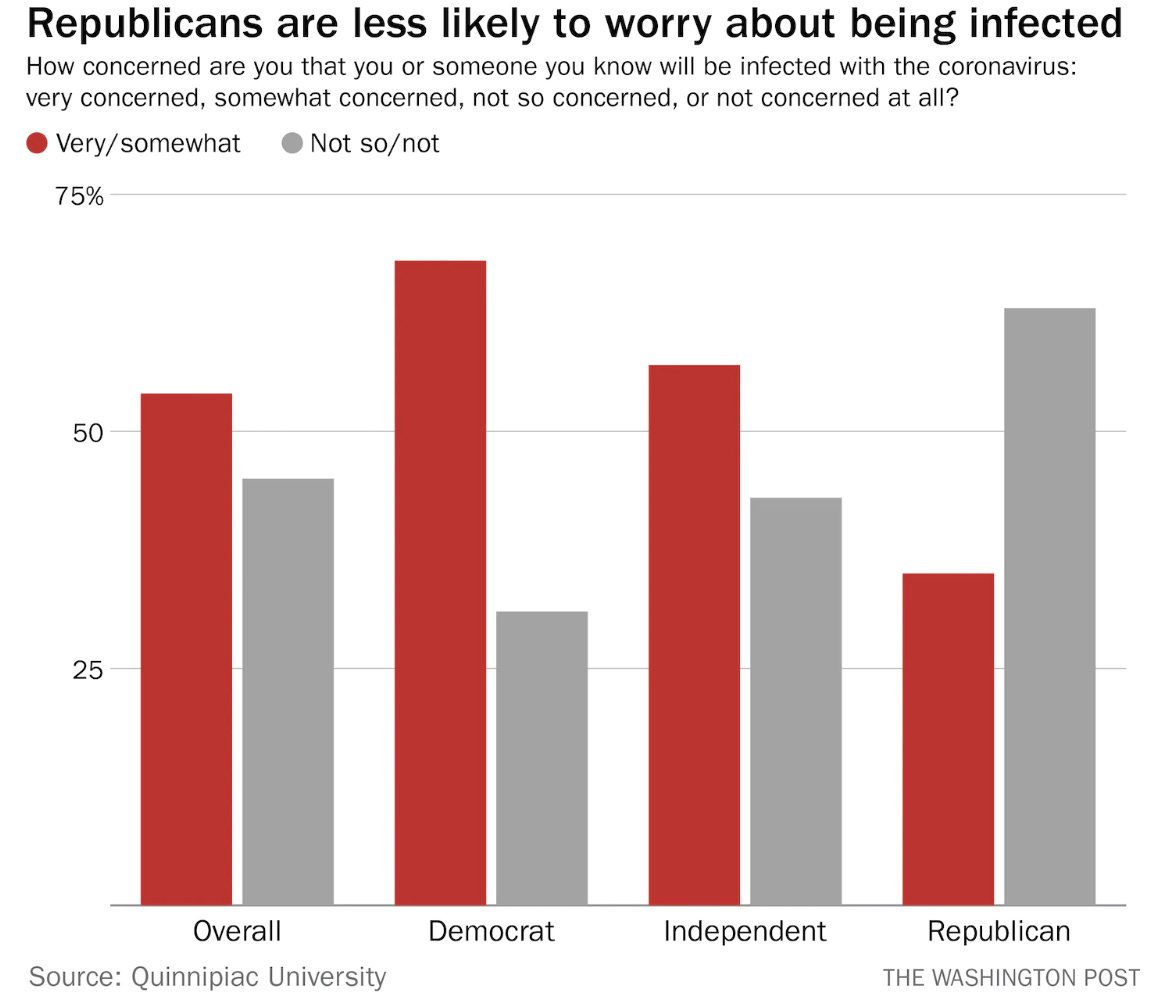
Trump's relentless disinformation has successfully politicized the crisis, with the disturbing results that Republicans are less likely to believe media reports or take the threat seriously:
"A lot of people will have this and it's very mild, they'll get better very rapidly."
Donald Trump interview on Hannity, March 4, 2020.
Trump still equates COVID-19 with flu, which he apparently thought was little worse than a bad cold. "I didn’t know people died from the flu," he said March 7th.
Trump said he learned this last week, more than two months into the crisis while meeting with the heads of the Centers for Disease Control and Prevention (CDC) in Atlanta, Georgia.
They told him normal flu sickens 34 million in the US in a season, with 350,000 hospitalizations, 20,000 deaths, and a mortality rate of 0.1% (CDC). The 2017 to 2018 season was the worst in four decades with 80,000 deaths and 900,000 hospitalizations in the US. Trump's own grandfather died in the 1918 Spanish Flu Pandemic.

By comparison, COVID-19 spreads faster and is 10x deadlier than flu, as testified to Congress by Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases and head of Trump's own coronavirus task force.
While Trump has downplayed and deliberately distorted the truth about the coronavirus threat, he also has restricted Dr. Fauci from speaking publicly and federal health officials from releasing vital data to doctors caring for patients, which has "hampered the U.S. government’s response to the contagion."
Trump is well known for dismissing expertise and input from seasoned specialists and credentialed advisors. He claimed last week the 3.4% fatality rate for COVID-19 projected by the World Health Organization (WHO) was a "false number" based on his no-evidence "hunch" that the true number “is way under 1%." He claimed a "natural ability" to understand disease metrics.
Trump has pronounced himself a "stable genius" who knows "more than anybody"—more than scientists, judges, economists, generals, and more—about pretty much every topic such as:
"More about renewables than any human being on Earth"(April 2016).
"More about courts than any human being on Earth" (November 2015).
"More about taxes...maybe in the history of the world" (May 2016).
"Nobody in the history of this country has ever known so much about infrastructure as Donald Trump" (July 2016).
Trump on January 22, 2020: "We have it totally under control."
Trump actually began to lose control of the crisis in 2018, 100 years after the pandemic that killed his grandfather.
That was when he gutted 80% of the US health security capacity and infrastructure including hundreds of millions in funding, firing leadership and staff, and eliminating entire departments.
Trump's goal was to make room for his flagship $1.4 trillion in tax cuts for corporations and the wealthy enacted the year before.
As a result, wrote Foreign Policy in January, the United States "has never been less prepared for a pandemic."
Ron Klain, who was the US Ebola response coordinator (2014-2015) correctly projected in The Atlantic in June 2018 "several large gaps in U.S. preparedness for the next global outbreak:"
“A leadership gap. “There is no one at the White House right now who is in charge of this problem,” Klain said.
A funding gap. “We’re underfunding, underinvesting” in preparedness, he said.
A facilities and training gap. Klain said that there was exhaustive training of first responders carried out right after the Ebola outbreak in 2014. But there are other diseases for which they are still unprepared. “Training needs to be renewed. People need to be drilled,” he said. “Our first responders need to be trained. We need better and more facilities.”
A science gap. “We haven’t yet developed all the vaccines and the therapeutics we need,” Klain added.
A policy gap. There are “holes in American law that we need to fill about licensing people in medical emergencies to practice in other states or,” he said, “using the Stafford Act”—the federal law that governs relief and emergency assistance for state and local governments during a natural disaster—“to respond to emergencies."
Absent these safeguards, Trump lies as did in spades on March 6 when US cases had escalated to 319 on the way to 1,663 and counting:
“[The coronavirus] came unexpectedly a number of months ago. I heard about it in China. We made a good move. We closed it down. We stopped it. Otherwise, uh, the head of the CDC said last night you would have had thousands of more problems if we didn't shut it down early. It was a very early shut down.”
As CNN’s Dr. Sanjay Gupta observed, “That’s clearly not the case.”
Yet it is true outside America, and has been for weeks.
Tom Hanks and his wife Rita Wilson just discovered they have COVID-19 while working in Australia, where “testing is free and widely available.”
Had they been back home in the States there’s a good chance they may have waited weeks to be tested, if at all.

Nevertheless, ready or not, the challenge of COVID-19 is here:
The American Hospital Association advised US hospital operators and health experts across the country in February to expect as many as "96 million cases in the US, 4.8 million hospitalizations, and 480,000 deaths associated with the novel coronavirus."
This tracks the midpoint of the estimates presented by Dr. Brian Monahan, the attending physician of Congress and the U.S. Supreme Court, who projected 70 million to 150 million cases in the U.S. in a closed-door meeting on Tuesday to Senate staff.
AHA warned hospitals to "prepare for an impact to the system that's 10 times greater than a severe flu season."
Dr. Fauci has projected a 15-20% serious illness rate among patients infected.
It won't take even that many to overwhelm US capacity. The US has only 2.8 hospital beds per 1,000 people, fewer versus Italy’s 3.2 beds per 1,000, China’s 4.3, and South Korea’s 12.3.
Ron Klain told MSBC on Tuesday there are 1 million hospital beds in the US overall, with 70% already filled with normal patients. This amounts to normal capacity of roughly 35 million patients per year.
Moreover, severe flu admissions tend to be multiple days to weeks, and there currently are only 65,000 ventilators in the whole country, most of which now are in use for this year's flu season.
Even the lowest estimated surge from COVID-19 can quickly overtax the system. Then what?
Well, for one, thing, patients with other maladies suffer from lack of care in the crunch. Klain said, "almost as many people often die, not from the epidemic but from the inability to get healthcare for other things."
Hospitals already have been short on masks, sanitizers, drugs, and other vital suppliers before the surge even began. Chronic staff shortages will only worsen.
Lack of testing remains a serious obstacle to measuring the pace of the virus spread in the US as well as timely patient care, owing to insufficient supplies of tests as well as inconsistent testing standards and protocols and even differences by location.
Trump has declared falsely that tests were widely available and everyone can get tested, that a "million" tests had been shipped out, and that the botched CDC test kits were "perfect."
None of that was true, and the situation only started to improve over the past week with just 13,000 tests completed so far by CDC and state public health labs.
South Korea has been testing 10,000 per day, and had completed 140,000 by early March when the US had tested only 1,500.
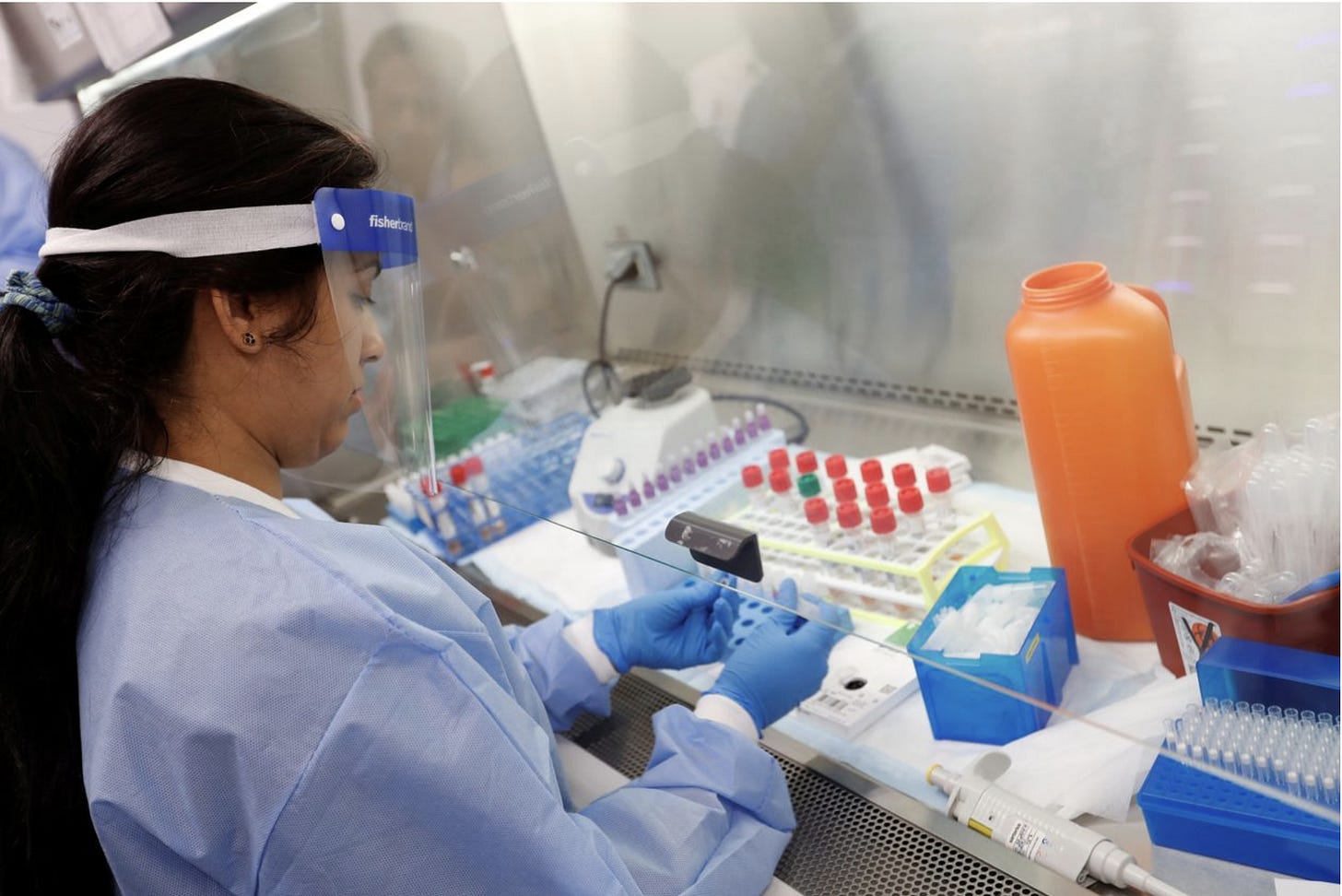
WSJ: The Food and Drug Administration has been working to ramp up the speed and quality of coronavirus testing after a slow and troubled start in the U.S./Reuters

The epidemic is likely to play out over months, potentially into next year
COVID-19 is a completely new strain of coronavirus, with no vaccine for at least a year and no evident cross-immunities as there are with the other coronaviruses.
It also is surprisingly resilient and pervasive: it can last in the air for 30 minutes, it can infect a victim 15 feet away, it can survive for 2-3 days on glass, fabric, metal, plastic, or paper at 98 degrees ambient temperature.
It can live in patients for five weeks after contagion.

For hospital operators and investors alike, this means months of uncertainty with substantial risk of disturbing headlines.
Hospitals can expect revenue and operating profits squeezed by spiking volumes of patients through the emergency room, their lowest margin operations, while high margin surgeries and discretionary procedures are postponed and even canceled.
First-quarter results already have been hit with a stronger than normal flu season this year, with second and potentially third-quarter results expected to be impacted by a broad-based surge of significant COVID-19 cases.
Operating profits are likely to be further pressured by higher than expected costs for labor and supplies. It's not confirmed how much if any federal aid will materialize for uninsured patients, numbers which already have been climbing before the COVID-19 crisis. Uncompensated care can claim 20-30% and more of gross revenue for hospitals in a "normal" year.
There goes half the year. Even if the epidemic tapers off by yearend, hospital operators are unlikely to recover sufficiently in the second half to meet rosy guidance for the year announced less than 2 months ago.
I expect HCA Holdings (HCA US), with its commanding market presence as the largest hospital operator in the US, with also the strongest margins and balance sheet, will be comparatively more resilient versus its weaker peers Tenet Healthcare (THC US) and Community Health Systems (CYH US).
That said, a substantial percentage of HCA's uncompensated care volumes are produced in Texas and Florida where vulnerable and uninsured populations are higher. I rate HCA bonds "underperform" on continued downside risk to pricing.
Tenet has traditionally trailed its larger peers with below-average hospital profits, which it has offset with aggressive diversification into surgery centers. This also makes it more vulnerable to the COVID-19 pressure to profits. I rate Tenet bonds "underperform" on continued downside risk to pricing.
Community Health continues to struggle to stay afloat with little margin for significant business shocks—it is the riskiest of the group. I rate Community bonds "underperform" on continued downside risk to pricing.
Contact Us:
Disclaimer
This publication is prepared by Bond Angle LLC and is distributed solely to authorized recipients and clients of Bond Angle for their general use. In addition:
I/We have no position(s) in any of the securities referenced in this publication.
Views expressed in this publication accurately reflects my/our personal opinion(s) about the referenced securities and issuers and/or other subject matter as appropriate.
This publication does not contain and is not based on any non-public, material information.
To the best of my/our knowledge, the views expressed in this publication comply with applicable law in the country from which it is posted.
I/We have not been commissioned to write this publication or hold any specific opinion on the securities referenced therein.
Bond Angle does not do business with companies covered in its
publications, and nothing in this publication should be construed as a solicitation to buy or sell any security or product.Bond Angle accepts no liability whatsoever for any direct, indirect, consequential or other loss arising from any use of this publication and/or further communication in relation to this document.